Coronavirus and
Lung Cancer:
Frequently Asked
Questions
Lung Cancer:
Frequently Asked
Questions
We want to hear from you. We are interested in knowing what topics we should cover in future updates.
Please share your thoughts with us by taking this short (1-2 minute) anonymous survey.
Learn more about coronavirus and its impact on people with lung cancer.
COVID-19 VACCINE
Is there a vaccine to protect me against COVID-19?
As of our December 14 update, the Pfizer/BioNTech vaccine had just been granted Emergency Use Authorization (EUA) by the FDA. On December 18, the FDA also granted an EUA to Moderna’s mRNA-based vaccine. As of January 6, approximately 5.3 million people in the US have received at least one vaccine dose, far short of the goal federal officials had set. Learn more about the prioritization of patients with cancer, vaccine comparison, and more in our January 11 update.
UNDERSTANDING THE CORONAVIRUS
How does COVID-19 spread?
COVID-19 is the disease caused by the new coronavirus, which is named SARS-CoV-2 (Severe Acute Respiratory Syndrome CoronaVirus 2).
What is the origin of the SARS-CoV-2 virus?
There has been a lot of speculation on the origin of SARS-CoV-2. Scientists have now confirmed that SARS-CoV-2 is not a genetically engineered virus, meaning it is not manmade.
What do the new COVID-19 variants mean?
There has been a lot of media attention around new variants of the virus. The short answer is we do not fully understand the implications and impact of these variants yet. More studies are needed to determine impacts on transmissibility, infectivity, disease severity, immune response, and vaccine efficacy. Knowing this, we must remain vigilant in practicing public health measures, increase efforts around contact tracing and identifying new variants, and rapidly increase vaccination efforts nationwide. Learn more in our January 11 update.
Who is at increased risk of developing a serious form of COVID-19?
Older populations and health-compromised groups may be at higher risk of getting very sick with COVID-19. Specifically, individuals with lung cancer, individuals with lung disease, such as COPD (chronic obstructive pulmonary disease), and individuals in active cancer treatments may be susceptible to a more serious form of the infection.
The Thoracic cancERs international coVid 19 cOLlaboraTion (TERAVOLT) registry study is specifically tracking outcomes for lung cancer patients infected with COVID-19. Recently published data from this study suggests that stage IV non-small cell lung cancer (NSCLC) patients are at higher risk of complications and mortality if they get infected with SARS-CoV-2. Of the patients included in the study, 33% succumbed to complications from COVID-19.
Another study from Memorial Sloan Kettering Cancer Center looked at a cohort of 423 cancer patients with COVID-19 (8% of which were lung cancer patients) and found that 20% developed severe respiratory illness (including 9% who required mechanical ventilation) and 12% died within 30 days. In addition, the authors found that administration of immunotherapy was associated with a higher risk of complications.
Both of these studies reinforce two points: cancer patients may be at a higher risk of developing complications from COVID-19 and various patient (such as lung damage from radiation therapy) and treatment-specific (immunosuppressive treatments such as chemotherapy) factors determine the extent of severity.
Which age groups have severe responses to COVID-19?
Recent data released by the CDC demonstrated that almost all age groups are susceptible to a serious form of COVID-19 that requires hospitalization.
This is especially important to keep in mind given that younger people have been more resistant to social distancing.
PREVENTING INFECTION
How does COVID-19 spread?
Individuals with COVID-19 appear to transmit the virus from their respiratory tract (e.g., when coughing) even when symptoms may be very minor. Although the infected person can still perform usual functions, they continue to be infectious. This explains why we are seeing widespread transmission in the community.
It is important to remember that infected individuals may not show symptoms of COVID-19 but can still spread the virus to others.
How long does SARS-CoV-2 survive outside the body?
A recent study found that the SARS-CoV-2 virus (that causes COVID-19) can survive up to four hours on copper, up to 24 hours on cardboard, and up to two to three days on plastic and stainless steel. This virus can hang out as droplets in the air for up to three hours before they fall. But most often they will fall more quickly.
Research suggests that transmission of SARS-Cov-2 is possible through aerosols and fomites (solid objects and surfaces that are able to carry pathogens and transmit infections).
What can I do to protect myself and my loved ones from COVID-19?
We encourage everyone to avoid travel and stay home unless it is for medical appointments (after calling and confirming with your doctor first), to get groceries, prescriptions, or other necessary supplies.
In general, follow best practices for public health, such as avoiding contact with other people, handwashing with soap and water for 20 seconds (or using a hand sanitizer), and respiratory etiquette including covering the mouth and nose during sneezing and coughing. Wearing masks or facial coverings have played a large role in preventing transmission of the virus. Many of the steps you would take to protect yourself from catching the flu also apply for protecting yourself against COVID-19.
Since the virus can spread through surfaces, we recommend that after you bring articles into your home, you do the following:
- Wash your hands after carrying delivered items into your home.
- After accepting a package that’s in a cardboard container, put it aside or in the garage and let it sit for a day or two before opening (if possible).
- After opening a package, wipe down all articles that have solid surfaces with chlorine wipes or disinfect with an alcohol-based solution.
- At this time, there is no guidance on how to disinfect edible items such as fruits and vegetables.
- Follow cleaning and disinfecting procedures listed on the coronavirus.gov website
What is social distancing and how do I practice it?
Social distancing is avoiding other people to help decrease transmission of a virus, like the one that causes COVID-19, within the community. It is now estimated that as many as 31% of new COVID-19 infections are being caused as a result of transmission through asymptomatic individuals – those who have been infected with SARS-CoV-2 but don’t shown signs and symptoms of the disease. This reinforces why we need to practice stringent social distancing to flatten the curve.
The Centers of Disease Control and Prevention (CDC) recommends maintaining a minimum distance between individuals of 6 feet or 2 meters. Other social distancing measures such as cancelling gatherings over 10 people and avoiding crowds can slow the spread of the virus and spread cases out over a longer period. This helps hospitals provide care while avoiding being overwhelmed by patients.
Earlier this year, many state and local governments issued “shelter in place” orders – meaning citizens should limit their travel for only essential work or medical care or buying groceries and obtaining medicines. Since then, many states have loosened restrictions and reopened certain businesses. Check your state and local government websites for more guidance about current requirements where you live.
As of September 7, new cases appear to be on a decline nationally, but pockets of high COVID activity remain. Read our September 7th update to learn more.
Is social distancing working?
Yes, it is working. The CDC continues to recommend social distancing to help decrease transmission of COVID-19 within the community. Social distancing measures, such as cancelling public gatherings and avoiding crowds, can slow the spread of the virus and spread cases out over a longer period of time, which can help hospitals provide care while avoiding being overwhelmed by patients. Social distancing helps “flatten the curve” in the spread of an infectious disease. We encourage you to check out CDC’s COVID-19 community mitigation strategies here.
Do I continue to social distance?
Yes, social distancing is a public health measure that can protect us from SARS-CoV-2. Social distancing minimizes risk of exposure to the virus. It is important to keep in mind that social distancing is NOT the same as social isolation. We encourage you to keep in touch with all your family, friends, and loved ones through phone and video conversations.
Social distancing is different from self-quarantine. Self-quarantine should be practiced by people who have been exposed to SARS-CoV-2 and who are at risk for coming down with COVID-19.
When can we resume normal activities in our lives?
The straightforward answer to that question is when we have achieved a reasonable level of herd (or community) immunity, which occurs when a high percentage of the community is immune to a disease through vaccination and/or prior illness (natural infection). Herd immunity is critical because it not only prevents the spread of infection but also protects people who may not be able to receive a vaccine.
Epidemiologists are hard at work figuring out what levels of herd immunity will protect us from SARS-CoV-2. Initial models suggested that the percentage of people who need to be immune to the virus to achieve herd immunity was around 70%. However, recent research suggests a lower threshold, on the order of only 40%. It is extremely important to keep in mind that no matter the threshold of immunity required, these estimates are based on mathematical models and not true population-based studies. Learn more about herd immunity in our August 24 update.
How can we celebrate the holidays safely?
With the year-end holidays around the corner and an anticipated increase in travel, the CDC has extended its travel advisory to include the winter break. We encourage our community members to weigh the risks and benefits of travel during this winter. Thanks to the vaccine, the end of the pandemic may be on the horizon. Till such time, maintaining public health measures such as masking, handwashing, social distancing, and minimizing non-essential travel are our best bets for protection.
In places or states with a high number of new cases, some experts even advise canceling (or at least postponing) holiday celebrations. You can check each state’s COVID-19 new case activity here and use a risk calculator to decide the level of risk.
How can I minimize exposure to SARS-CoV-2 when restrictions are lifted?
Easing restrictions does not mean we should stop maintaining public health precautions. We highly recommend that everyone:
- Wear masks in public. A recent publication in the Proceedings of the National Academy of Sciences shows wearing masks is protective, given that transmission of the virus through air is one of the primary means of infection.
- Continue to maintain six feet distance from others in public
- Continue to practice social distancing
- Self-quarantine in case you suspect you may have been exposed to the virus
- Wash your hands regularly with soap and water
- Avoid touching your face
- Avoid large gatherings of people
- Minimize all non-essential travel
As a lung cancer patient or caregiver, if you have any questions on how to maintain public health measures as you run errands and go to work, please check out the CDC resources here. We are also learning about the long-term effects of an infection. Impact of COVID-19 on the body can last for several months. In some extreme cases, damage to the lungs is severe enough to require a double-lung transplant. We therefore firmly believe that it’s better to be safe than sorry!
Should I travel within the United States? Do I leave my city to go to someplace safe — such as a rural area?
Though the CDC does not typically make suggestions about domestic travel, they highly recommend avoiding all non-essential travel within the US. Several cities and states already have a shelter-in-place order. Check out these points to keep in mind should you need to consider domestic travel.
Likewise, you should not be leaving your urban apartment or home and move to a rural area for many reasons. Do not indulge in “disaster gentrification” for your own safety, the safety of your loved ones, and that of other community members. It is our duty to keep rural communities insulated from this disease as much as possible.
Should I use homemade masks to protect myself?
Yes, CDC reports that a significant portion of individuals with COVID-19 lack symptoms (“asymptomatic”) and that even those who eventually develop symptoms (“pre-symptomatic”) can transmit the virus to others before showing symptoms. This means that the virus can spread between people interacting in close proximity, even if those people are not exhibiting symptoms. In light of this new evidence, CDC recommends wearing cloth face coverings in public settings where other social distancing measures are difficult to maintain (e.g., grocery stores and pharmacies) especially in areas of significant community-based transmission.
Masks should be worn in conjunction with maintaining adequate social distancing. It is also important to keep in mind that these face masks are not surgical masks or N95 masks (to be used primarily by healthcare works as part of personal protective equipment).
Where are the best recommendations for my safety?
Rely on information from reputable sources, including the CDC and World Health Organization websites.
What is herd immunity?
Herd immunity (or community immunity) occurs when a high percentage of the community is immune to a disease through vaccination and/or prior illness. We currently face several challenges to achieving herd immunity. First, seropositivity rates remain significantly below the ~70% required to achieve herd immunity, even in hotspot areas such as NYC. Second, a growing number of reports suggest that antibody levels fall off significantly as early as 8 weeks after infection (though other features of the immune system may provide some protection).
How risky is returning to “normal” activities?
These updates are intended to give you the latest evidence on what we know and to provide a framework for you to make your own decisions as we all learn how to navigate this new “normal.” In that spirit, we share this recent graphic that helps assess the relative risk of various daily activities.
COVID-19 SYMPTOMS, TESTING, AND TREATMENT
What are the symptoms of COVID-19?
Symptoms may appear 2-14 days after exposure and may include fever, tiredness, dry cough, and shortness of breath. Some patients may have aches and pains, nasal congestion, runny nose, sore throat or diarrhea. Patients may present with non-respiratory symptoms even before they have respiratory symptoms. Gastrointestinal symptoms such as anorexia, diarrhea, vomiting, and abdominal pain may show up even before respiratory symptoms of COVID-19. Also, conjunctivitis may be present in a small subset of patients as well. These symptoms are usually mild and begin gradually.
Some may become infected but don’t develop any symptoms and don’t feel unwell, though these asymptomatic individuals can still transmit the disease.
What should I do if I think I have COVID-19? How do I get tested?
If you (as a patient) or a loved one (a caregiver) exhibits the symptoms of COVID-19 (including but not limited to fever, dry cough, shortness of breath), immediately follow self-quarantine procedures. Immediately contact your healthcare provider (could be your primary care physician) about whether you need to get tested. Your healthcare provider will be able to guide you on next steps. The CDC and the Association of Public Health Laboratories maintain a list of laboratories that are currently conducting COVID-19 tests. If you are having difficulty breathing, please go directly to the Emergency Department.
Please remember that you may not have symptoms even if you are infected with SARS-CoV-2. Social distancing is the only way to avoid getting infected with the virus. As a caregiver, please take extra precautions when you need to leave your house or apartment.
What types of treatments or vaccines are available for COVID-19?
On December 11, the United States Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the first SARS-CoV-2 mRNA vaccine, BNT162b2, manufactured by the pharmaceutical giant, Pfizer. The New York times reported that large-scale manufacturing and distribution of vaccines has already begun, with the first dosing to start on December 14, 2020. Read our December 14 update to learn more.
If you or your loved one (caregiver) has a confirmed diagnosis of COVID-19, your/their healthcare provider will be the right person to decide what type of treatment is useful. Please do not treat COVID-19-related symptoms without consulting your healthcare provider. Do not try to procure or hoard medications such as hydroxychloroquine that are approved for use in other conditions, as this is creating a shortage of these medications for patients with conditions for which the drugs are already approved.
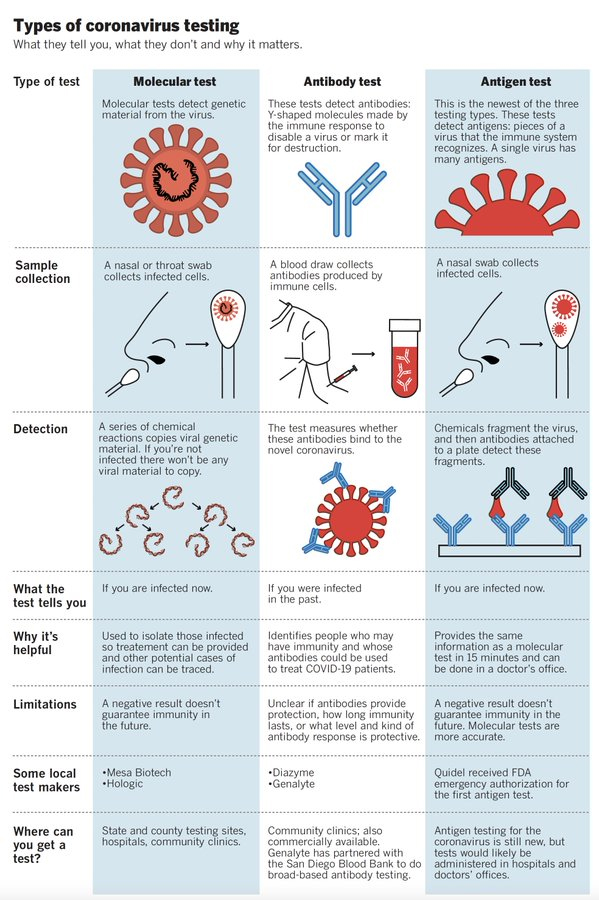
What types of coronavirus testing are there for both active and past infections?
Currently, active infections are tested using a nasal swab test. The FDA also recently approved a rapid antigen detection test to identify actively infected cases. Past infections are identified through serological (blood) tests that detect antibodies against the SARS-CoV-2 virus.
This infographic shows the differences between the tests used for the virus that causes COVID-19. Read our May 18 update and watch a short interview with Dr. Nicolas Vabret, Assistant Professor of Medicine, Hematology and Medical Oncology at Icahn School of Medicine at Mount Sinai, to learn more.
{kind=link}
Should I get tested for COVID-19? Which test is right for me? What do the test results mean?
If you or your loved one suspects that they have been exposed to SARS-CoV-2, and/or have developed the three most common COVID-19 symptoms (fever, cough, and shortness of breath), we recommend you get tested.
Currently, three tests are available for COVID-19. The choice of test depends on whether you suspect that you have an active (existing) infection, or you were infected in the past and want to confirm infection.
Learn more about the different types of testing in our July 13 update.
If I had COVID-19 and have now recovered, will I become immune to SARS-CoV-2?
The answer is – we do not know. When an individual is infected with a pathogen, such as bacteria or a virus, typically the body mounts an immune response. This is true even in individuals who remain asymptomatic. The immediate immune response ensures that the pathogen is eliminated from the body, and immunological memory (the basis of vaccination) ensures that if the body encounters the pathogen in the future, the immune system is ready to fight it off.
It is not currently clear whether a one-time infection with SARS-CoV-2 confers lifetime immunity against the virus. Scientists are still evaluating what level of immunity is needed to confer protection against future infections with SARS-CoV-2. New research out of China suggests that the antibody response (a measure of immunity) to SARS-CoV-2 infection may not last as long as for other respiratory viruses, particularly among asymptomatic patients. The study, published in Nature Medicine, suggests that antibody levels fall off by over by 70% in both asymptomatic and symptomatic patients by 8 weeks following infection. Though the sample size is small, if true, these results have important implications for establishing “herd immunity” (also sometimes referred to as community immunity) through natural infection as well as vaccination efforts.
Has the SAR-CoV-2 virus mutated? Is this new mutation more infectious? What does this mean for prevention, vaccines, and treatment?
A preliminary manuscript (which has not yet undergone peer review) describes the emergence of a new mutation seen in a specific gene of the SARS-CoV-2 virus. This mutation, which was first discovered in Europe, is called D614G. It causes an increase in the number of spike proteins in the virus. Since the spike protein is how the virus attaches to human cells, the authors concluded that this mutation makes the virus more infectious. However, it does not appear to make the resulting disease more severe or deadly. Currently, the real-world implications of this mutation and its impact on the development of vaccines and treatments are still unclear.
Are blood tests detecting coronavirus antibodies more frequently?
Many countries are using blood tests to look for SARS-CoV-2 antibodies in their populations. Testing of blood serum is called serology. The percentage of individuals in a population that have these antibodies in their blood serum is called seroprevalence. As COVID-19 spreads across the globe, different areas will have different levels of seroprevalence.
The CDC is now conducting large-scale geographic seroprevalence surveys at a number of sites across the country. Initial results from the first six sites showed rates of people who tested positive for SARS-CoV-2 antibodies varied from about 1% (in WA state) to about 7% (in greater NYC area).
Click here to learn more about recent studies.
TELEHEALTH IN THE ERA OF COVID-19
What is telehealth?
The terms “telehealth” and “telemedicine” are used interchangeably to describe using telecommunications technologies to deliver health care. It includes a variety of services that deliver health care, public health, and health education, and ranges from methods as simple as telephone calls and email to live video, mobile apps, remote patient monitoring and uploading scan images. The Center for Connected Health Policy (CCHP) provides an excellent overview of telehealth here.
How is the use of telehealth changing during the COVID-19 pandemic?
In light of the COVID-19 pandemic, federal and state policies are rapidly adapting to allow for greater utilization of telehealth services. The Centers for Medicare & Medicaid Services (CMS) have created some useful fact sheets highlighting various policy changes, including this one summarizing Medicare telemedicine services and this one addressing sweeping regulatory changes to meet patients’ needs during this time. Private health insurance companies are also modifying their policies to enable greater use of telehealth.
CCHP is maintaining an updated list of COVID-19 telehealth coverage policies.
What are some of the barriers to broad uptake of telehealth during the current crisis?
The challenge with adapting telehealth policies in real-time to address an unfolding and unprecedented public health crisis is that, in a pre-COVID-19 world, federal and state policies varied widely in how telehealth services were provided and covered.
Most of the current challenges relate to regulatory and reimbursement issues, including licensure requirements. Even as the popularity of telehealth among patients grows, private healthcare payers have been slow to embrace the technology. The Federation of State Medical Boards is maintaining an updated list of states currently waiving telehealth licensure requirements.
The “digital divide” is also a barrier to accessing telehealth. Patients who are elderly, in areas with poor Internet or cellular coverage, or economically disadvantaged, may not be able to access the technology necessary to telehealth.
How do I know if I am eligible to obtain telehealth services? What can I do to ensure broader access?
Again, laws vary by state regarding how telehealth is being implemented and what health insurance companies and providers can do. Review your health insurance plan benefits and policies frequently to learn how they may be changing. This CCHP list of COVID-19 state actions may also be helpful.
CCHP also monitors state and federal telehealth legislation to provide a clear overview of policy across the nation. As a citizen, you can monitor legislation that has been introduced in your state and testify to show your support or opposition. You can call your legislators to ensure your needs are being heard.
For a great overview and more in-depth discussion on all of these points on telehealth, please check out GO2 for Lung Cancer’s Rapid Response Living Room from April 14, 2020, featuring Dr. Joelle Fathi.
How is the FDA allowing the use of telehealth for lung cancer clinical trials?
The FDA allows for changes to be made to the clinical trial protocol without prior FDA review or approval if the change is intended to protect the life and well-being of the patient. Therefore, changes in protocol conduct necessary to immediately assure patient safety, such as use of telehealth for safety monitoring instead of on-site visits, can be immediately implemented once the new protocol has been approved by an IRB. The FDA can then be subsequently notified. It is important to note that the consult is just one part of patient safety monitoring. The patient’s clinical trial team and the clinical trial sponsor will also need to have a clear plan in place to ensure that patient safety is prioritized in case routine monitoring such as blood tests and heart function exams are unable to be conducted.
CONSIDERATIONS FOR PEOPLE WITH LUNG CANCER
Should I keep appointments with my oncologist or for treatment?
If you have an oncology visit due in the next couple of months, please contact your treating physician as soon as possible to discuss the right approach for you. They may respond with option to reschedule or switch to a virtual appointment.
Virtual appointments are not appropriate for infusions for chemotherapy or immunotherapy, or potentially critical scans. Talk to your doctor about your medications and whether you should/can get extra supplies.
The oncology community has come up with the following suggestions for lung cancer treatment. Please be advised that these recommendations are subject to change.
- If you are a patient with a confirmed diagnosis of small cell lung cancer (SCLC), you may not wish to delay any additional diagnostic procedures (such as imaging and biopsies) or treatment (such as chemotherapy and radiation). You and your doctor should discuss what’s right for you.
- If you are an early-stage non-small cell lung cancer (NSCLC)patient (Stage I to IIIB):
- Who has already had surgery, your doctor may decide to not start with adjuvant chemotherapy and/or radiation
- Who has not yet had surgery, you and your doctor may decide to wait on the surgery. Also, instead of surgery, radiation may be an option
- Who is currently on chemo-radiation, your doctor may decide to continue with your treatment or wait on additional treatment
- If you are an advanced-stage non-small cell lung cancer (NSCLC)patient (Stage IIIC and IV):
- Who is on a targeted therapy (pill), you may continue with your treatment as planned. Make sure to check with your doctor and pharmacist to ensure an adequate supply of your cancer medication
- Who is already on immunotherapy or chemotherapy, your doctor may decide to continue with your treatment or wait on additional treatment. They may decide to have you receive infusions at your local clinic or even home infusion, as needed
- Who is already undergoing radiation therapy, your doctor may choose to hold off on additional treatment or keep you on treatment as planned, based on your individual health situation
All treatment decisions should be made jointly by you and your doctor. Do not change your treatment plan or doctor’s visit without consulting your doctor first. Telehealth or remote consults may be an option for checking in with your doctor. Click here to learn more. Also, there may be the option to be referred to a “COVID-19-free” hospital or treatment center.
Should I keep other healthcare appointments?
In every case, you should contact your healthcare provider and inquire about your appointment.
Should I get a flu shot?
We are strongly recommending that all eligible patients and caregivers get their annual flu shot as soon as possible, as it takes approximately two weeks from receiving the shot to have adequate protection.
Public health experts are particularly concerned about the potential for patients to get infected with both influenza and SARS-CoV-2 this winter. Additionally, since the symptoms for these two viruses are similar, many patients experiencing flu-like symptoms may flood already overtaxed healthcare systems.
Some patients, particularly those on checkpoint inhibitors, may be concerned about whether they can take the flu shot – we always recommend asking your doctor but previous studies suggest that it is safe for patients.
How is the pandemic impacting lung cancer research?
Lung cancer research has continued in full swing. This year’s virtual World Conference on Lung Cancer’s Presidential Symposium featured three fantastic Phase III trial presentations on immunotherapy for non-small cell lung cancer (NSCLC), a new targeted therapy for ALK-positive lung cancer, and immunotherapy for mesothelioma. Click here to learn more.
In every case, you should contact your healthcare provider and inquire about your appointment.
What is the impact of COVID-19 on new cancer diagnoses?
A new study showed an alarming overall drop (46%) in new cancer diagnoses across six different tumor types, including lung cancer, for the period from March 1 to April 18, 2020. Additional reports from the across the country indicate an even higher drop in new cancer diagnoses. The COVID and Cancer Research Network reported a decline of 74% across 20 sites in the US for April 2020 compared to April 2019.
We want to empower you with a set of questions to ask your doctor in advance of any visits so that you feel they are taking appropriate precautions to ensure your safety. Read these questions in our August 10 update.
What are the implications of COVID-19 for my personal cancer treatment?
As a result of the COVID-19 pandemic, doctors and scientists are reevaluating treatment schedules and the “usual way of doing business.” One example is the recent April 28, 2020 FDA approval for a new dosing regimen for the immunotherapy drug, pembrolizumab. This approval is based on data presented at the 2020 AACR Virtual Meeting.
Dr. Jacob Sands, a leading lung cancer medical oncologist at Dana-Farber Cancer Institute, provides a nice discussion on the importance of individualized lung cancer management in the COVID-19 era here.
Read our May 4 update to learn more.
How is COVID-19 affecting the conduct of clinical trials?
The US Food and Drug Administration has recently issued guidance to help clinical trial sponsors figure out the best approaches to ensure that trials can proceed within resource-constrained settings. This may include the use of telehealth for safety monitoring instead of on-site visits in some cases.
If you are part of a clinical trial, we recommend you discuss your trial participation immediately with your research team.
If you were considering enrolling in a clinical trial, you may want to discuss with your treating physician what options are available for you. Any decision about trial participation should be made jointly by you and your healthcare team.
Please note that LungMATCH, our treatment option personalized service remains available. Our specialists are partners on your treatment journey—clarifying options, referring you for molecular testing directing you to appropriate clinical trials, and following up with you after treatment begins. Given the situation, our specialists are confirming availability of trials before recommending them. To get started, call us at 1-800-298-2436 or email support@go2.org.
Can patients receive their clinical trial drug through home delivery?
The FDA understands that there may be a risk of exposure to SARS-CoV-2 when a patient visits a clinical trial site. In case a patient is receiving their drug (such as a targeted therapy pill) through their clinical trial site pharmacy, the clinical trial sponsor now has the option of directly mailing the drug to the patient’s home as long as the following conditions are met:
- The patient already takes the pill at home as part of the trial protocol
- The shipment of the drug to the patient’s home does not affect the chemical nature of the drug
- The sponsor keeps a clear track of number of pills shipped to the patient’s home and is able to share this information with the FDA when asked
This is an extremely important question for the lung cancer community — where clinical trials often require an infusion of a chemotherapy, an immunotherapy, an angiogenesis inhibitor, or a combination of the above.
The FDA understands and appreciates that a patient may be exposed to SARS-CoV-2 when they travel to their routine clinical trial infusion center. Therefore, the FDA is open to alternative sites for administration (e.g., home nursing or alternative sites closer to a patient’s home where the infusion is given by trained medical personnel who are not part of the study team). The ultimate decision to allow this switch to home infusion or local infusion is based on the following criteria:
- The shipment of the drug to the local infusion center or to the patient’s home does not affect the chemical nature of the drug
- The sponsor keeps a clear track of the amount of shipped to the patient’s home and is able to share this information with the FDA when asked
Another option is delaying or discontinuing infusion for a period of time while the patient continues to be on the study. This decision needs to be made jointly by the clinical trial team and the patient.
Note: The ultimate decision on whether to allow a home infusion or local infusion is highly dependent on the drug being tested. Some infusions cannot be given at a local infusion center or through home infusion. Examples include drugs that require ability to manage potential infusion reactions with specific medication, or treatments such as gene therapy or cell therapy that require exacting handling procedures and patient monitoring.
What are the recommendations/guidelines for how I should change my screening or care during the pandemic?
Various professional societies/organizations have created consensus statements to ensure lung cancer patients continue to receive the best care possible during this crisis. These statements are a testament to the way the global oncology community is working together to support and protect the lung cancer community. Click here to read a brief summary of what different professional societies are saying about COVID-19 and lung cancer treatment.
What are the impacts of COVID-19 on the state of academic cancer research?
Most academic research institutions, including universities and hospitals, have shut down most research labs and closed enrollment in some clinical trials to accommodate government-imposed shelter in place mandates and protect researchers’ lives. Only critical research, such as maintaining cell lines or animal models for preclinical research and some clinical trials with strong evidence of effectiveness, is being allowed to continue. These are institutionally mandated restrictions that have been put into place to protect university staff.
Funders of academic lung cancer research in the US such as the National Cancer Institute, the Department of Defense, and private non-profits (e.g., LUNGevity Foundation, GO2 for Lung Cancer, Lung Cancer Research Foundation, Lung Cancer Foundation of America) have all made concessions to accommodate the needs of the scientific community and best support investigators during this critical time, while trying to minimize any delays in lung cancer research.
How is the pandemic impacting lung cancer research?
Lung cancer research has continued in full swing. This year’s virtual World Conference on Lung Cancer’s Presidential Symposium featured three fantastic Phase III trial presentations on immunotherapy for non-small cell lung cancer (NSCLC), a new targeted therapy for ALK-positive lung cancer, and immunotherapy for mesothelioma. Click here to learn more.
How has the COVID-19 pandemic impacted oncologists and the cancer healthcare community?
The impact of the COVID-19 pandemic on the mental health of oncologists cannot be underestimated. Several studies suggest that oncologists will likely suffer from “burn-out” syndrome and post-traumatic stress disorder (PTSD). As patients and advocates who work regularly and intimately with oncology healthcare professionals, we must not forget to express our gratitude to all members of the patient care team.
What is the latest data on risk of COVID-19 for lung cancer patients?
We are still learning about how patient-specific factors and treatment-specific factors related to lung cancer can influence the severity of COVID-19. It is best to discuss how an individual patient’s situation will be impacted with the treating physician.
What is abundantly clear at this point is that multiple studies point to increased risk and worse outcomes in lung cancer patients with COVID-19. As the pandemic continues to spread throughout the US, it is imperative that lung cancer patients continue to take the threat seriously and take appropriate steps to protect themselves and those around them.
Several real-world studies that addressed overall risk for cancer patients as well as lung cancer in particular were presented at the recent American Association of Cancer Research “COVID-19 and Cancer” virtual conference on July 20-22, 2020. Read our July 27 update to learn more.
Do lung cancer patients infected with COVID-19 have worse outcomes?
COVID-19 presents a unique threat to all cancer patients, especially those with lung cancer. Various international efforts are underway to understand these risks and what it means for patients and their cancer care. As states continue to reopen, it is important not to let your guard down and to maintain all the precautions you have been taking over the past few months. This virus has not gone away and it is important that you and your loved ones take appropriate steps to minimize exposure.
Click here to read our June 1 update for more information.
How can I tell if information I read about COVID-19 is reliable and how do I make sense of contradictory information?
In the era of COVID-19 when information is evolving rapidly — with new information being available daily — it is important to depend on trusted and reputable sources of information. We recommend that you follow information from trusted and medically vetted websites such as the CDC, the WHO, and the IASLC. Information on how to access these websites are included in the Resources and websites section below.
It is incredibly important to verify sources of your information to ensure that we are not spreading false information which can not only cause unnecessary panic but can be downright harmful (such as misinformation regarding drugs). A good resource that provides guidelines to evaluate health information can be found here.
When judging what you read from publicly available sources, we suggest you use the Evidence-Based Medicine (EBM) Pyramid as a guiding framework. Read our May 4 update to learn more.
What other resources on COVID-19 are available to me?
- The National Cancer Institute has a special website for COVID-19 and emergency preparedness. Coronavirus: What People with Cancer Should Know
- We are following updates provided by the World Health Organization (WHO) and the US Centers for Disease Control and Prevention (CDC), which can be found here:
- https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen
- https://www.cdc.gov/coronavirus/2019-ncov/index.html
- IASLC’s Guide to COVID-19 and Lung Cancer
- Johns Hopkins Coronavirus Resource Center is one of the best places to get current updates.
- Interactive map of US COVID-19 cases by state
- The One-Two Punch: Cancer And Coronavirus (an important perspective for cancer patients)
- You can find information specific to your state or city or town on your health department’s website.
- A list of state department of health websites can be found here
- A list of local health department websites can be found here
- The American Medical Association is also maintaining a resource website for healthcare providers.
.